Recently, at a forum where I am involved, a poster asked about evidence for non-transitioning therapies for transsexuals. Now on that forum are a tiny number who consistently pound an anti-transition drum. But as I demonstrated in my reply, their position is not congruent with the position of the medical community today. Here is what I wrote, with minor edits to make it more appropriate for this blog.
__________________________________________________
The AMA is now overwhelmingly on board with fundamental brain differences being the root cause of transsexuality. And the APA (both of them) both state that the most effective therapy statistically for transsexuals is transition.
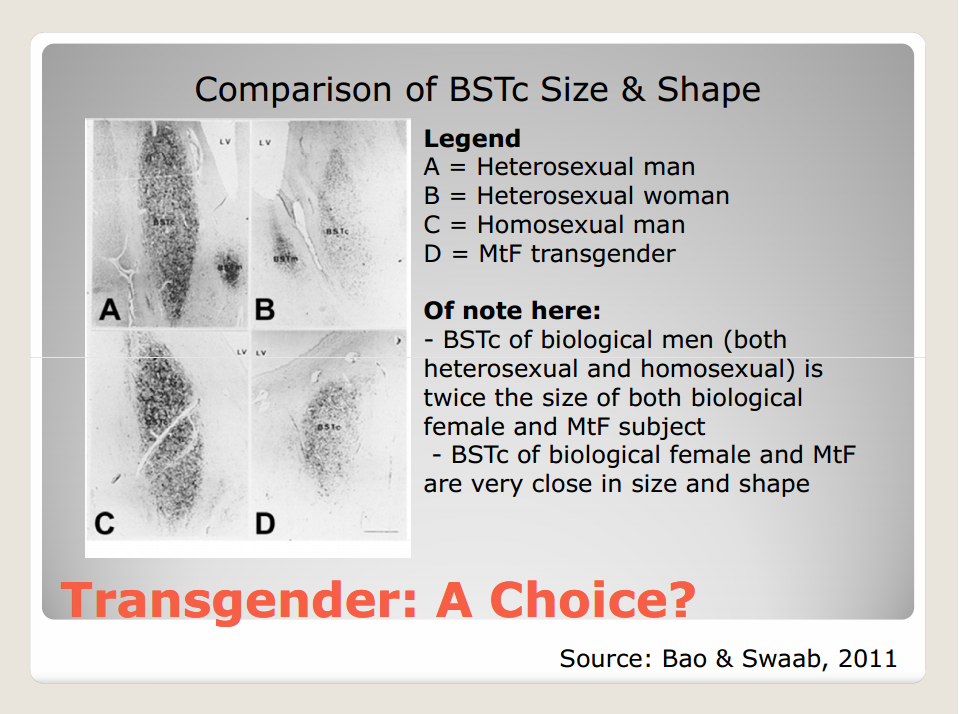
One of the most important of these is brain differences concerns the BST in the hypothalamus. “In the hypothalamus, the bed nucleus of the stria terminalis (BST) is thought to be important for gender identity. One study showed that male-to-female transsexuals had decreased BST staining identical to that for genetic XX female subjects (8). In contrast, genetic XY male subjects had significantly increased BST staining. BST staining was not influenced by sexual orientation or sex hormone levels.”
These differences can be seen below:
In addition, further brain structure differences are being identified as well that impact transsexuals.
This NIH document references the study (by van Kesteren PJ, Gooren LJ, Megens JA. An epidemio-logical and demographic study of transsexuals in The Netherlands. Arch Sex Behav. 1996;25:589–600) that sex reassignment as overwhelmingly statistically successful in addressing the needs of the transsexual community. Given the size of the TS community the size of the study is significant. If the rates of transsexuality are as high as 1 in 600 as has been suggested by various studies, and if 1 in 2500 actually undergo SRS which have been suggested by direct analysis of number of surgeries in the US per year, then the size of the study in question was almost 25% of the SRS population of the Netherlands and 3% of the overall Netherlands TS population. If the rates of transsexuality are lower, then the size of the study is even more significant because it represents an even larger cross section of the TS population!
Here is the NIH position:
Quote
__________________________________________________
Treatment options for patients with gender identity at variance with physical appearance can be evaluated in the order of extent of invasiveness. The least invasive intervention would be counseling such patients to accept the circumstance. As already noted, however, no available data support the success of such therapy. The next least invasive approach might be a targeted treatment of the underlying problem. The medical community, however, has little knowledge about the brain region associated with gender identity, and even less is known about techniques for manipulating it.Although current transgender treatment is relatively invasive and does not address the problem completely, it is the most successful intervention available. Studies report very high transgender patient satisfaction with sexual reassignment. Thus far, the largest evaluation has been a survey of Dutch transgender patients (10). Among the 1,285 patients surveyed, 1,280 were satisfied.
__________________________________________________
As noted, “no available data support the success” of counseling patients to simply accept their circumstances. The second discussed option, manipulating the brain to become more accepting of the body, is not currently possible because the “medical community, however, has little knowledge about the brain region associated with gender identity, and even less is known about techniques for manipulating it“.
This leaves transitioning as the primary therapy for dealing with GID. As has been noted in the past here, there are people who do manage to live out their lives without transitioning to live in a new gender role. Good for them. But they are also the statistical minority among patients suffering from significant GID. For that category of patients, the number one therapy of choice today is transitioning (aside from suicide and I think we all agree that suicide is a bad option, yes?).
Therapists will assist a patient in trying to meet their personal goals but a transsexual suffering from significant GID ought to be prepared to discover that non-transitioning treatments are very likely to fail to bring them to a level of comfort with themselves that allows them to live a full and fruitful life. Certainly there will be those cases that do succeed at this, but as the NIH document notes, the medical community’s primary treatment therapy today is transition, including HRT, and optionally including surgeries to further assist the body to conform to the expectations of the mind.
Therefore, in answer to the original poster’s question – you are unlikely to find any large scale answer to your question of non-transitioning treatments that work. In almost every case where that does occur, the patient has developed their own unique regimen for coping with their GID that is specific to that patient. The single treatment option that does work and which is medically and statistically supported at this time by the medical and psychiatric and psychological communities is transition.
To the original poster, if you choose to not transition, it’s pretty much you and your therapist in uncharted waters. It’s possible you will succeed. Good luck if you choose that path. I will not dissuade you from taking whatever path you choose but I will stand by the statements in this post that transition is the proven most effective treatment for transsexuals suffering from severe GID.
P.S. This is the reason that there is so-called “cheerleading” for transition in the community – because it works. And because it is overwhelmingly statistically successful. Those are facts.
__________________________________________________
The above was the body of my response in that discussion thread.


You must be logged in to post a comment.