The following was put together by Transadvocate, a trans advocacy website, on their Facebook page. In order to not lose track of it, I am putting it here. This is not my work! I am copying it for ease of reference! Thank you Transadvocate and Rehan! If I find another link to this, I will add it here for completeness as well.
In regards to the Crossift HQ refusal of Chloie Jonnson’s participation at the games here are some facts that should be considered before any sensationalistic claims are made without proper knowledge.
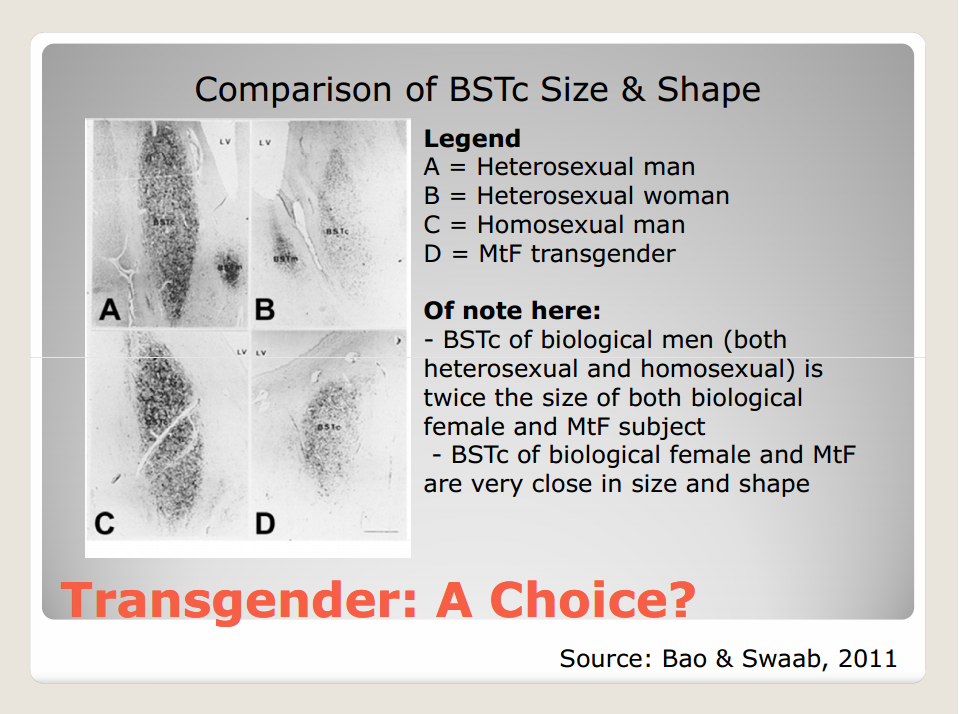
First of all the XY vs XX argument is invalid and not sufficient. There are well documented cases of XX males and XY females. The SRY gene region is normally found on the Y chromosome but is not a reliable method of testing since not only is not always found on the Y chromosome it also triggers a gene cascade not well understood by scientists yet that in turn affect other tissues during development which may lead to altered sexually dimoprhic traits in individuals, such as brain structure.
This is evidenced by scientific literature cited
Male-to-Female Transsexuals Have Female Neuron Numbers in a Limbic Nucleus
http://press.endocrine.org/doi/abs/10.1210/jcem.85.5.6564
and
Sexual differentiation of the human brain: relevance for gender identity, transsexualism and sexual orientation
Read More: http://informahealthcare.com/doi/abs/10.1080/09513590400018231
http://informahealthcare.com/doi/abs/10.1080/09513590400018231
and
Sexual Differentiation of the Bed Nucleus of the Stria Terminalis in Humans May Extend into Adulthood
http://www.jneurosci.org/content/22/3/1027.short
and
A sex difference in the human brain and it’s relation to transsexuality.
http://depot.knaw.nl/821/1/15106_285_swaab.pdf
with subsequent study by Dr.Swaab et al. And Kruijver et al. showing differences in the Bed Nucleus of the Stria Terminalis, SDN, Hypothalamus and gray matter volume underlining the importance of brain physiology.
http://www.sciencedirect.com/science/article/pii/0165380688902313
http://www.sciencedirect.com/science/article/pii/S1053811909003176
http://www.tandfonline.com/doi/abs/10.1300/J082v28n03_07#.UxoCwRbPPFI
http://books.google.ca/books?hl=en&lr&id=JFpq6hYQRhQC&oi=fnd&pg=PA41&dq=brain+dissection+transgender+Dr.+Swaab&ots=FjtewJ28wz&sig=8F-QOG1Q5QCEIMe1oQwqlWNb9ko#v=onepage&q&f=false
http://www.hawaii.edu/PCSS/biblio/articles/2005to2009/2006-atypical-gender-development.html
Also studies showing it to be irreversible
http://aace.metapress.com/content/nm510264636815vk/
There is also an article linking hormone related genes to the atypical sexual dimoprhism. Genes CYP19 (Aromatase responsible for testosterone to estrogen conversion), AR (androgen receptor, the “key” hole for the cell that the testosterone “key” acts on to elicit it’s effects) and ESRB (Estrogen Receptor Beta which is responsible for the initiation of differentiating gene cascades in the fetal brain during fetal hormonal “washes”)
here
http://www.sciencedirect.com/science/article/pii/S0306453005000454
Continuing on the topic of performance and gender testing the IOC released a statement before the 2012 summer Olympics.
“The new rules state that a panel of independent medical experts will examine through a blood test the testosterone levels in a woman and will then make a recommendation about whether she could be eligible to compete.”
The IOC and NCAA have decided after extensive research (independently) that Hormone profile is the primary determining factor for gender qualification in sport.
The Olympics requires 2 years post surgery before being allowed to compete at an INTERNATIONAL event.
The NCAA requires only one year of HRT.
This was determined the minimum to not have any unfair advantage as evidenced by the quotes from respective authorities below.
“Requiring sex reassignment surgery before allowing participation for the high school or collegiate student athlete is medically unnecessary and not linked to competitive equity IOC regulations requiring surgery for Olympic transgender athletes have been controversial and it would be unreasonable to”make this requirement for high school and college students”
ERIC VILAIN M.D., PH.D., PROFESSOR, DIRECTOR OF THE CENTER FOR GENDER-BASED BIOLOGY AND CHIEF MEDICAL GENETICS DEPARTMENT OF PEDIATRICS, UCLA
“Research suggests that androgen deprivation and cross sex hormone treatment in male-to-female transsexuals reduces muscle mass; accordingly, one year of hormone therapy is an appropriate transitional time before a male-to- female student athlete competes on a women’s team
ERIC VILAIN: M.D., PH.D., PROFESSOR, DIRECTOR OF THE CENTER FOR GENDER-BASED BIOLOGY AND CHIEF MEDICAL GENETICS DEPARTMENT OF PEDIATRICS, UCLA
“Transgender student athletes fall within the spectrum of physical traits found in athletes of their transitioned gender, allowing them to compete fairly and equitably”
DR. NICK GORTON
AMERICAN BOARD OF EMERGENCY MEDICINE, MEDICAL LEGAL CONSULTANT, TRANS HEALTH CARE
Further more, the difference need to be put into perspective when transgender women are compared with cisgender women they fall within a female range after the required time period (1 year NCAA, 2 years post-op IOC).
“Differences within the sexes are considerable and often times larger than differences between the sexes ”
DR. WALTER BOCKTING, PH.D.
PRESIDENT OF WPATH, ASSOCIATE PROFESSOR, UNIVERSITY OF MINNESOTA MEDICAL SCHOOL
These facts are presented based on scientific literature as cited
here
Elbers JM, Asscheman H, Seidell JC, et al. Effects of sex steroid hormones on regional fat depots as assessed.
here
Australian Sports Commission. Transgender in sport.www.ausport.gov.au/fulltext/2001/ascpub/women_transgender.asp (accessed 22 Mar 2005).
here
as contrasted between these two
↵ Stamm R, Veldre G, Stamm M, et al. Dependence of young female volleyballers’ performance on their body build, physical abilities, and psycho-physiological properties. J Sports Med Phys Fitness 2003;43:291–9. [Medline][Web of Science]
↵ Viitasalo JT. Anthropometric and physical performance characteristics of male volleyball players. Can J Appl Sport Sci1982;7:182–8. [Medline]
and here
Pilgrim J, Martin D, Binder W. Far from the finish line: transsexualism and athletic competition. Fordham Intellectual Property Media & Entertainment Law Journal2003;13:495–549.
And the rest of these studies
↵ Federation Internationale de Volleyball. Medical regulations, ed. 2004. http://www.cev.lu/mmp/online/website/main_menu/downloads/file_28430/fivb_med_regulations_-_revised_7.pdf (accessed 23 Mar 2005).
↵ Lausanne Declaration on Doping in Sport (adopted by the World Conference on Doping in Sport). 1999.www.sportunterricht.de/lksport/Declaration_e.html (accessed 23 Mar 2005).
↵ Ritchie I. Sex tested, gender verified: controlling female sexuality in the age of containment. Sport History Review2003;34:80–98.
↵ Batterham AM, Birch KM. Allometry of anaerobic performance: a gender comparison. Can J Appl Physiol1996;21:48–62. [Medline]
Thomas JR, French KE. Gender differences across age in motor performance: a meta-analysis. Psychol Bull1985;98:260–82. [CrossRef][Medline][Web of Science]
↵ Shepard RJ. Exercise and training in women. Part I. Influence of gender on exercise and training responses. Can J Appl Physiol2000;25:19–34. [Medline][Web of Science]
↵ Dickinson BD, Genel M, Robinowitz CB, et al. Gender verification of female Olympic athletes. Med Sci Sports Exerc 2002;34:1539–42. [CrossRef][Medline][Web of Science]
↵ Simpson JL, Ljungqvist A, de la Chapelle A, et al. Gender verification in competitive sports. Sports Med 1993;16:305–15. [Medline][Web of Science]
↵ Introducing the, uh, ladies. JAMA1966;198:1117–18.
↵ Doig P, Lloyd-Smith R, Prior JC, et al. Position statement. Sex testing (gender verification) in Sport. Canadian Academy of Sports Medicine. 1997. http://www.casm-acms.org/PositionStatements/GendereVerifEng.pdf (accessed 23 Mar 2005).
There is no “residual” advantage and often times transgender athletes are at a disadvantage due to severely lowered testosterone levels in comparison to native females. Cisgender women have a higher testosterone than transgender women who have had reassignment surgery and the related information.
http://transathletes.org/hormones.php
Other issues that arise in the form of practicality
1) Her numbers pale in comparison to other female athletes
Crossfit profile comparison between her and CLB:http://games.crossfit.com/compare/161983/8404
Back Squat: 225 lb Clean & Jerk: 165 lb Snatch: 125 lb Deadlift: 275 lb
These numbers pale in comparison to the top competitors as well as compared to many other regional athletes.
2) Let her compete, if she has an unfair advantage it will be very apparent and provide evidence for these as of yet unfounded claims of unfair advantage. There are yet to be any instances of a transgender athlete dominating competitions if this were to be so likely.
3) Saying this will open the door for other males to “become” transgender and dominate is very short sighted. Firstly they would have to adhere to the strict protocol involving Hormone Replacement Therapy which would remove that advantage. Secondly transgender people face a MASSIVE amount of discrimination not to mention the amount of money and physical pain of procedures that need to be endured to complete the requirements. The transgender suicide rate is 41%, forcing someone to live as the opposite identity is devastating psychologically and would also be true of someone trying to “fake” it. (Remember once the surgery is done it is a PERMANENT change, is winning crossfit that important?)
4) Having larger bone structure and lowered muscle mass constitutes a disadvantage.
5) Furthermore there is no consistent testing policy in crossfit for PED’s. A cis-female using AA has a much larger and much more distinct advantage which could be considered universally as an “unfair advantage”.
The most shocking thing is the completely deplorable and inappropriate reply from Crossfit HQ, who seem to be the ones lacking in understanding of the human genome and biology.

You must be logged in to post a comment.